
Understanding Your Lipid Profile: What do each of the metrics mean?
Your lipid profile reveals key insights about cholesterol, triglycerides, and lipoprotein(a), helping us tailor a plan to protect your heart health.
Zohaib Iqbal
3/17/20265 min read

What your lipid profile means — and what actually matters for your heart health
Cholesterol is not simply “good” or “bad”. It is an essential molecule, vital for cell structure and for the production of hormones and vitamin D. The body produces cholesterol naturally, and it circulates in the bloodstream within particles called lipoproteins.
Some of these particles, such as LDL, can contribute to plaque build-up in the arteries, while others, such as HDL, are involved in transporting cholesterol away.
What matters is not just your cholesterol level, but the type and behaviour of these particles over time, and what this means for your individual cardiovascular risk.
This guide is designed to help you understand what your results mean — and, importantly, what they do not mean.

Why your cholesterol results matter
Cholesterol is carried in the blood by particles called lipoproteins. Some of these particles can enter the walls of arteries and contribute to the gradual development of atherosclerosis — the process that underlies heart attacks and strokes.
This process develops silently over many years. Blood tests allow us to assess this risk early, often long before symptoms occur.
However, interpreting these results properly requires more than looking at a single number.

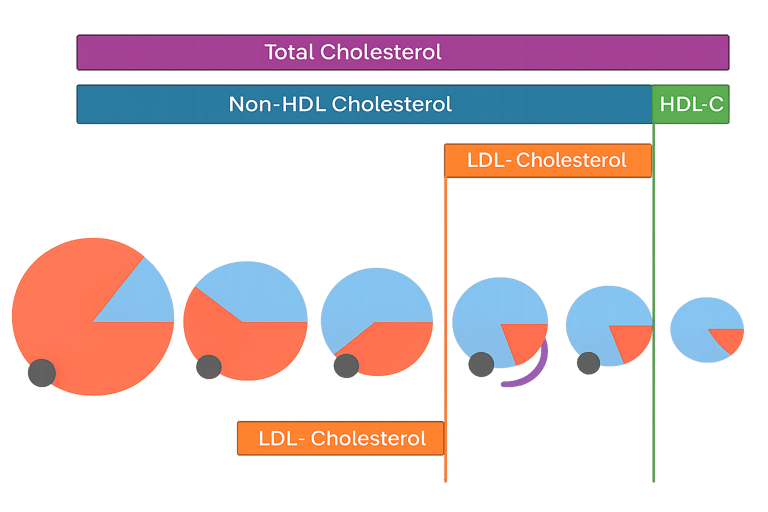
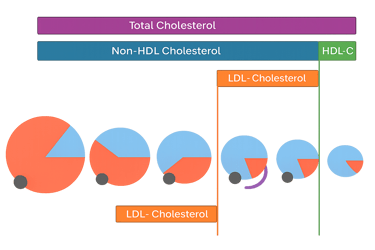
Total Cholesterol
This is the overall amount of cholesterol in your blood.
While it is often the number patients focus on, it is not particularly helpful on its own. This is because it includes both harmful and non-harmful components.
A “normal” total cholesterol does not necessarily mean your risk is low, and a “high” result does not always mean treatment is required.
The components of a lipid profile
LDL Cholesterol
LDL cholesterol is the one of the most important markers when assessing long-term cardiovascular risk.
It represents the cholesterol carried within low-density lipoprotein particles (LDL particles), which transport cholesterol in the circulation. These particles can penetrate the inner lining of arteries, where they become trapped and trigger inflammation, leading to the gradual formation of atherosclerotic plaque.
Importantly, it is not just the cholesterol itself but the number of LDL particles over time that drives risk. The more LDL particles circulating in the blood, and the longer they are present, the greater the cumulative exposure of the artery wall.
For this reason, LDL cholesterol remains the primary target of lipid-lowering therapy. Robust evidence shows that reducing LDL cholesterol leads to a proportional reduction in heart attack and stroke risk, with benefits increasing the earlier and longer it is controlled.
HDL Cholesterol
HDL cholesterol is often referred to as “good” cholesterol, but its role is more nuanced than simply being protective.
It represents cholesterol carried within high-density lipoprotein particles, which help remove cholesterol from artery walls and return it to the liver (reverse cholesterol transport). Higher levels are associated with lower cardiovascular risk at a population level.
However, HDL itself is not a treatment target. Trials have shown that raising HDL cholesterol does not reduce cardiovascular risk, highlighting that particle function is more important than the absolute level.
HDL cholesterol also reflects recent metabolic and dietary exposures, integrating fat intake over preceding days as well as alcohol intake, weight, and insulin sensitivity. Levels can therefore fluctuate and act as a marker of how the body is handling lipids in real time.
Low HDL cholesterol is a recognised component of the diagnostic criteria for metabolic syndrome and typically reflects underlying insulin resistance rather than a primary disorder of HDL.
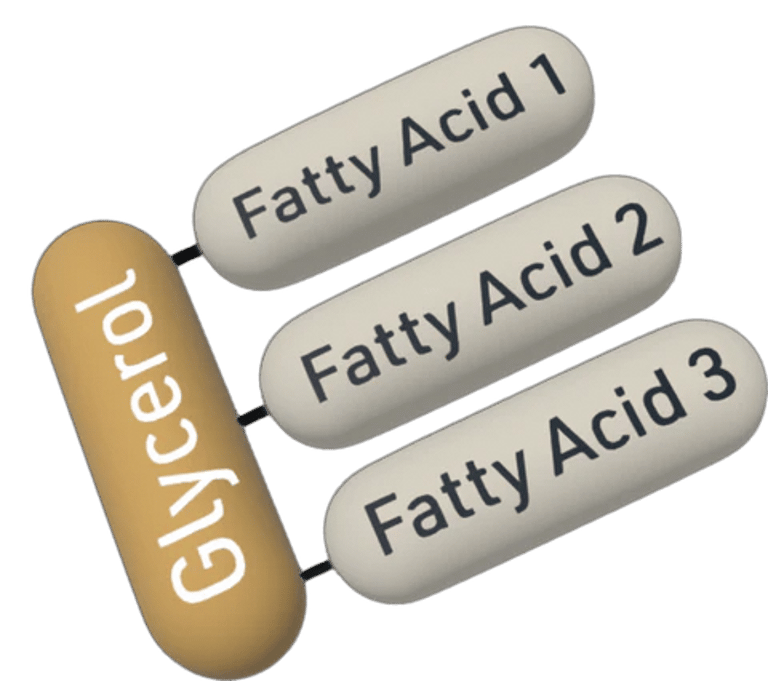
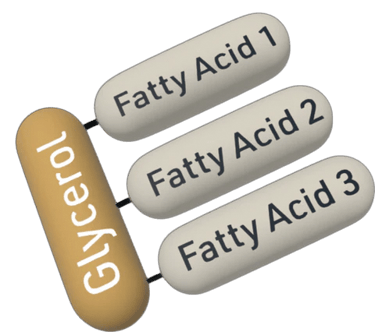
Triglycerides
Triglycerides are a form of fat carried in the blood and reflect how the body handles excess energy. After eating, surplus calories — particularly from sugars and refined carbohydrates — are converted into triglycerides and transported within lipoproteins.
Raised triglycerides are commonly associated with insulin resistance and often occur alongside excess weight, impaired glucose control, and certain dietary patterns.
In practical terms, triglyceride levels are often one of the most responsive parts of a lipid profile. They can improve significantly with changes in diet, weight, alcohol intake, and physical activity. However, persistently elevated levels may indicate an underlying metabolic issue and should be interpreted in the context of the overall lipid profile and cardiovascular risk.
Non-HDL Cholesterol
Non-HDL cholesterol is a highly informative measure of all the “atherogenic” cholesterol in the blood and is increasingly used to assess cardiovascular risk.
It is calculated by subtracting HDL cholesterol from total cholesterol and therefore captures the cholesterol carried in all potentially harmful lipoproteins, including LDL, VLDL, IDL, and remnant particles. These particles all have the ability to enter the artery wall and contribute to plaque formation.
Non-HDL cholesterol is particularly useful in people with raised triglycerides or metabolic conditions, where LDL cholesterol alone can underestimate risk. In this context, it provides a more complete picture of the total burden of cholesterol carried by atherogenic particles.
For this reason, UK NICE guidance currently stipulates non-HDL cholesterol as the primary treatment target in routine clinical practice, recommending at least a 40% reduction from baseline following initiation of lipid-lowering therapy. Lowering non-HDL cholesterol reflects a reduction in all harmful lipoproteins and is associated with a meaningful reduction in long-term cardiovascular risk.
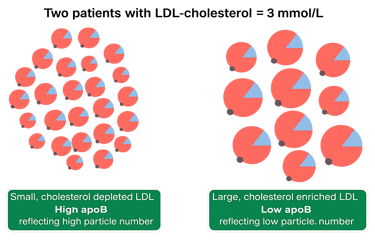
Apolipoprotein B (ApoB)
ApoB is one of the most informative markers in lipid assessment.
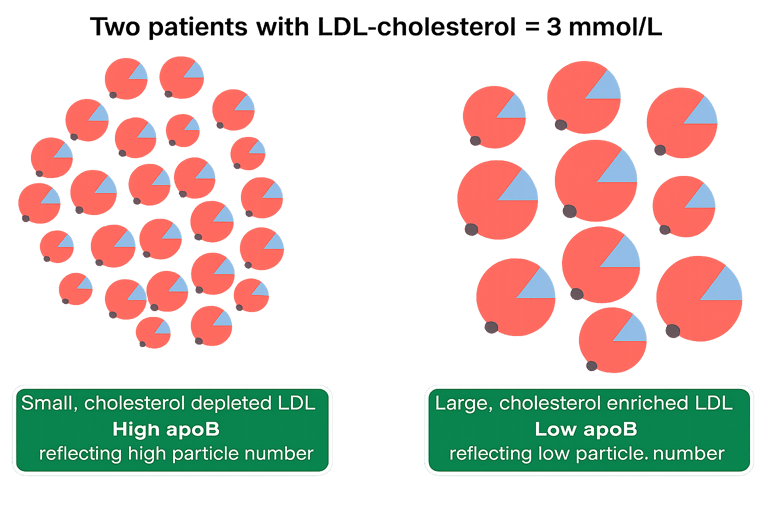
Rather than measuring how much cholesterol is present, it reflects the number of atherogenic particles in the blood — the particles that can contribute to plaque formation.
Each of these particles carries one ApoB molecule, so ApoB gives a direct measure of particle number.
In many cases, ApoB provides a more accurate assessment of cardiovascular risk than LDL cholesterol alone.
Lipoprotein(a)
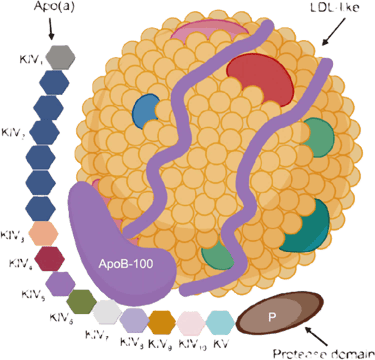
Lipoprotein(a), often written as Lp(a), is a genetically determined lipoprotein particle that is present from birth and remains relatively stable throughout life.
Structurally, it is similar to an LDL particle but with an additional protein called apolipoprotein(a), which gives it unique pro-atherogenic and pro-thrombotic properties. This means it not only contributes to plaque build-up in arteries but may also promote clot formation.
Lp(a) is a well-established independent risk factor for cardiovascular disease, and its levels are largely unaffected by diet, lifestyle, or standard lipid-lowering therapies. As a result, individuals can have a healthy lifestyle and normal routine cholesterol levels but still carry significant risk if Lp(a) is elevated.
Importantly, Lp(a) is not included in standard cholesterol testing, so many people are unaware they have elevated levels. When identified, it can help explain cardiovascular risk that appears disproportionate and may influence the intensity of risk factor management and screening of family members.
Recent UK stroke guidance now recognises the clinical importance of Lp(a), recommending that it should be considered in individuals—particularly under the age of 60—who present with ischaemic stroke or TIA without an obvious cause, with markedly elevated levels prompting specialist referral
Contact
GMC Registered | NHS Consultant Endocrinologist
For Patients
© 2026. All rights reserved.
For Healthcare Professionals
Book a Consultation
Refer a Patient